





Last week this tweet came across my feed and was widely and justifiably retweeted:
It became clear to me, that nephrology needed a similar essay:
Dr. Katie Kwon answered my call. Her essay:
My first foray into Twitter was about five years ago. Twitter was in the news a lot and I kept coming across online articles filled with viral tweets that were funny, pithy, and current. Those articles made Twitter seem like a virtual Algonquin Round Table. However, my first login didn’t look anything like that. Twitter asked for my email address book, then signed me up to follow people I already knew. I didn’t have the first idea how to go about seeing tweets from strangers on topics I found interesting. It was all too much work, and I quickly gave it up.

Then I attended ASN 2013. Since starting my nephrology training, I’ve tried to go every other year. I’m in private practice with two other colleagues, so ASN is my biannual chance to chat with other nephrologists. Slowly, painfully, I’ve grown my professional network. At first I would meet up with other alumni from my fellowship program and the faculty. Then, when our dialysis units were acquired by a small chain, I got to meet some other medical directors from around the country. It was nice to attend meetings knowing more than three people. But I knew I’d get a lot more out of ASN if I knew more people, and could learn their viewpoints on the presentations I was attending.
At the 2013 meeting, I had the opportunity to meet Joel Topf. He’s a nephrologist that I had long admired for his blog, and I had made comments on several of his posts that I particularly liked. He sent me a message that he was presenting a poster at ASN, so I decided to stop by. His poster was about the use of social media in nephrology, an area where’s he’s an influential evangelist. After our conversation, I signed up for a new Twitter account.
This time, the experience made a little more sense. I learned that one’s Twitter feed is determined by who you follow. I started by following Joel and then anyone else he tweeted at. Pretty soon I had a nice stream of commentary from nephrologists from many different countries, most of it focused on the ongoing meeting. I began to notice the hashtags and how you could also search for those to pick up the threads of a conversation about a particular topic.
Using my iPhone, I carefully pecked out a few tweets about the presentations I attended. I tried to tweet pearls that normally I would have written down in a notebook, rarely to be seen again. I was delighted when these tweets got starred and retweeted by new followers. It was even more exciting when respected faculty members, whose names I knew from journal articles, would add their thoughts and provide links to additional material. It enhanced the learning from each session I attended. I wound up with a deeper understanding and different perspectives. I even made a few real-life acquaintances and met some for lunch. It was the most productive ASN meeting I’d ever attended.
Returning home, my Twitter use became much more sporadic. I had set up the app to send me a notification if a lot of the people I followed tweeted about a particular topic. In this way I learned about some breaking trials and other events in the broader field of medicine, including the MOC debate. I rarely tweeted my own content, but Twitter is very forgiving of long periods of inactivity. You won’t lose followers as you might if you took a break from blogging. When I did have something to contribute, or a question to ask, it was easy to jump right back in. I discussed a few tough cases on the Nephrology On Demand forum, which I learned about from Twitter.
I returned to ASN for the 2015 meeting. This time I was able to start tweeting right away – thankfully, my phone remembered my Twitter password. I started by reading the comments from other people attending the plenary session. Their annotations and insights deepened my understanding of a topic that would otherwise be intimidatingly basic science in its orientation. I followed many more conference attendees who seemed to have valuable things to say. Then I realized that I could virtually attend multiple simultaneous sessions. This was great! I no longer had to miss talks that seemed interesting but conflicted with others I also wanted to see. I learned about great presentations on exciting topics as they unfolded in real time, and sometimes switched rooms midway through a session. The conference felt more dynamic and I was confident I was spending my time there wisely.
One session on Friday focused on the ongoing battle over MOC and the ABIM. This was a topic I had continued to follow for the past few years, and I was disappointed that it was so sparsely attended. However, the low turnout wound up having an unexpected benefit, which was a clear field for me to tweet about it. I tried to sum up each main point the speakers made, then highlight the comments from the audience. This was the first time my tweets seemed to resonate. My followers retweeted my reporting to their followers, and my audience grew. The instantaneous feedback that what I was doing had interest and value was fun and exciting.
I left ASN this year having met interesting colleagues across the country, both virtually and in real life. (Twitter is a great way to get people to visit your poster at ASN.) I picked up some tips to organize my feed, which made it easier to participate in the Nephrology Journal Club the next week. The discussion was about the SPRINT hypertension trial. It felt like being back in fellowship again, in a good way. I got to benefit from the analysis of hundreds of colleagues, both those who participated and through the links to commentary that they provided. I am in the process currently of writing a talk for our local primary care doctors about SPRINT, and the Twitter conversations I participated in are providing great material for my analysis.
Twitter has allowed me to connect with many more nephrologists than I would have managed to meet through more conventional means. Those relationships have real value, helping me stay current in my field and giving me varying perspectives on controversial topics. While I love my practice in a small Midwestern town, Twitter has provided the discussions that I enjoyed during my training years in a big academic center. I feel more connected to my profession and my practice of medicine will only continue to improve as a result of my participation.
Quick start to Twitter as a nephrologist:
- Sign up. Keep your Twitter name short; 140 characters goes quick and a long name uses up more of them.
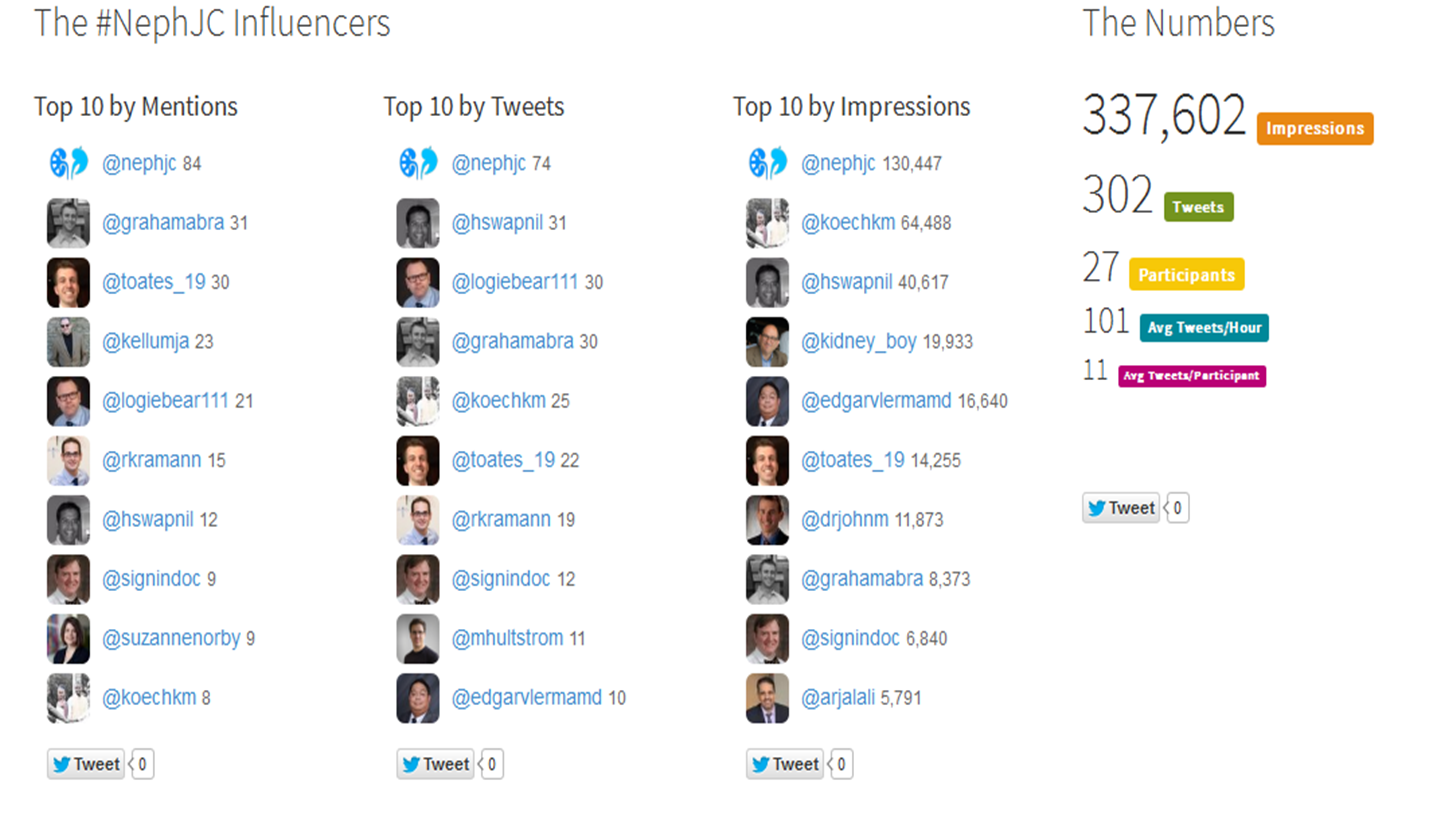
- Follow Nephrology Journal Club (@NephJC) and note the time of the upcoming discussion.
- Use tchat.io in your browser to follow the #NephJC discussion. Follow anyone who tweets something interesting. When you follow someone all of their Tweets show up in your feed. hand picking your feed will make Twitter more useful.
- Unfollowing is easy and it’s not fraught with emotion, unlike defriending on Facebook. Sometimes you’ll follow someone, only to find that the majority of their tweets are in a different language that you don’t understand. Unfollow them! If your feed is cluttered with irrelevant tweets, Twitter gets to be a slog.
- If someone is writing about an interesting topic marked with a #hashtag, just click on the hashtag to see other tweets with that hashtag. You can pick up more interesting people to follow.
- Start to tweet. Retweets are easy; bonus for adding your own viewpoint. Tweet about meetings or lectures you attend. You’ll get more out of it than jotting down notes you won’t read again. People will ask you questions or offer more resources. Your learning just doubled!
- It’s the internet; some people are weird, rude or hostile. Twitter has a block feature that prevents a person from reading your tweets or communicating with you. I don’t hesitate to block anyone who bothers me. I don’t want to use up any emotional energy worrying about a fleeting online interaction.
- Nephro-Twitter is a friendly place. If you start a message with someone’s username (i.e, @KatieKwonMD) your tweet will go directly to their feed, but not to your other followers. If you include their username in the body of your tweet, all your followers can see it. Reach out to people, ask them questions, point them to links you think might interest them. That’s how interesting conversations start.
















{kind=link}