
NephJC 10 post discussion
Tuesday, June 2nd 2026, 9 pm Eastern on X and Bluesky
Kidney Int. 2026 Apr 23:S0085-2538(26)00305-4. doi: 10.1016/j.kint.2026.03.015
Clinical and histologic predictors of non-diabetic kidney disease in patients with diabetes mellitus
TN Caza, V Charu, DF Dai, VG Davis, F Boyd, L Spenst, PD Walker
PMID: 42034202
Audio Abstract: https://audioscholar.cc/pdf/q2brtw2u7b?t=0
Introduction
Diabetic nephropathy (DN) has long been recognized as the leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) worldwide, correlating with the escalating global prevalence of diabetes mellitus (Zouh et al, Lancet, 2024). Historically, the clinical paradigm assumed an inevitable progression of renal decline in diabetic patients, characterized by a predictable transition from hyperfiltration to overt proteinuria and eventually ESKD. However, the advent of modern nephroprotective therapies has altered this natural history (Afkarian et al, JAMA, 2016), making atypical clinical courses more common and questioning the assumption that all kidney dysfunction in these patients is solely attributable to diabetes. It is increasingly recognized that patients with diabetes frequently develop non-diabetic kidney disease (NDKD), either as an isolated pathology or superimposed on underlying DN (Fiorentino et al, Nephrol Dial Transplant, 2017).
Recent global literature highlights that the prevalence of NDKD among diabetic patients undergoing kidney biopsy is remarkably high, frequently ranging from 18% to over 62%, depending on the specific cohort and biopsy thresholds utilized (Zeng et al, BMC Endocr Discord, 2022). The accurate identification of NDKD is critical because it dramatically alters a patient's prognosis and therapeutic trajectory. Many secondary diagnoses, such as acute interstitial nephritis, IgA nephropathy, or crescentic glomerulonephritis, are potentially reversible with targeted interventions like immunosuppression. Consequently, identifying and treating these conditions can significantly delay or entirely prevent the onset of ESKD.
Despite the high prevalence of NDKD, routine kidney biopsy is not universally performed in this population, and clinicians often face a diagnostic dilemma when evaluating kidney function impairment in diabetics. While emerging non-invasive diagnostic models and clinical predictors such as a short duration of diabetes (e.g., less than five years), the absence of diabetic retinopathy, active urinary sediment (hematuria), and acute, rapidly progressive renal failure provide valuable guidance, they cannot replace the definitive diagnostic utility of a tissue biopsy.
Currently, there are no established, universal guidelines dictating precisely when to perform a renal biopsy in a patient with diabetes for the identification of underlying non diabetic kidney disease. To address this critical knowledge gap Caza et al (Kidney Int, 2026) present the largest retrospective cohort study till date of patients with diabetes who have undergone native kidney biopsies, comprising 49,075 cases. By leveraging this unprecedented dataset, this study aims to robustly quantify the true frequency of NDKD, map the distribution of specific histopathological diagnoses, and identify the clinical indications and demographic parameters that significantly increase the odds of discovering NDKD.
Figure 2 a. Clinical spectrum of CKD in diabetes b.Cellular pathophysiology of kidney disease in diabetes from Anders et al, Nature Reviews, 2018
The Study
Methods
Study Design
This study represents the largest retrospective analysis till date of native renal biopsies from patients with diabetes. The research was conducted following institutional review board (IRB) approval and utilized a vast database of biopsies received at Arkana Laboratories (Little Rock, Arkansas, USA) between 2001 and 2024.
Cohort Development and Characterization
The study population was derived from a primary database of 229,026 native kidney biopsies. From this pool, 78,886 biopsies (34.4%) were identified as originating from patients with a clinical history of diabetes mellitus.
To ensure diagnostic accuracy and specimen adequacy, cases with fewer than 10 glomeruli by light microscopy were excluded. This resulted in the finalization of two primary cohorts:
Cohort 1 (n = 49,075): This large-scale cohort was utilized to determine the overall frequency of non-diabetic kidney disease (NDKD), the distribution of specific renal diagnoses, and the clinical morbidities present at the time of biopsy.
Cohort 2 (n = 13,995): A subset of Cohort 1, this group consisted of patients with biopsy-proven diabetic nephropathy (DN) where the specific clinical indication for the biopsy was available. This indication was determined through a meticulous manual review of clinical data, including age, gender, ethnicity, and the specific diagnosis the clinician intended to rule out.All kidney biopsies in diabetic patients were included from 2001-2013. From 2013 to 2024, the first 1000 biopsies in patients with DM were included every year.
Clinical Subset (n = 400): A subset of consecutively diagnosed patients was further analyzed for granular clinical parameters, including serum creatinine, quantitative proteinuria at presentation, and inpatient versus outpatient status.
Figure S1. Cohort diagram of patients included in the study. Caza TN et al, Kidney Int, 2026
Histopathological Evaluation
All renal tissue samples underwent comprehensive processing for light microscopy, immunofluorescence, and electron microscopy using standard diagnostic techniques. The pathologic evaluation included:
RPS Classification: Diabetic nephropathy was graded according to the Renal Pathology Society (RPS) classification system by a single pathologist
Chronicity Indices: Quantitative assessment of global glomerulosclerosis, segmental glomerulosclerosis, interstitial fibrosis and tubular atrophy (IFTA), arteriosclerosis, and arteriolar hyalinosis
NDKD Identification: All non-diabetic renal lesions were recorded, whether they occurred in isolation or concurrently with diabetic nephropathy
Clinical Indications for Biopsy
Clinical indications were self-reported by the treating clinicians and categorized for Cohort 2. These indications included:
Acute Kidney Injury (AKI)
Acute Nephritic Syndrome
Rapidly Progressive Renal Failure
Isolated Hematuria
Suspected NDKD
Proteinuria significantly greater than expected for the degree of DN
Chronic Kidney Disease (CKD) of unclear etiology
Analysis of Outcomes and ESKD Progression
To evaluate the long-term prognostic impact of NDKD, biopsy results were integrated with the United States Renal Data Service (USRDS) database (data available through 2022). Renal survival and progression to end-stage kidney disease (ESKD) were compared across three groups:
DN alone
DN with concurrent NDKD
NDKD alone
Kaplan-Meier survival analysis was performed for cases collected between 2001 and 2019, ensuring a minimum of 3 years of follow-up for outcome evaluation.
Statistical Analysis
Descriptive statistics (means, SDs, counts, and percentages) were used to summarize the data. The association between clinical exposures and outcomes was evaluated using:
Odds Ratios (ORs): With 95% confidence intervals (CIs) to assess the likelihood of NDKD based on clinical indications.
Breslow-Day Test: To evaluate heterogeneity among ORs.
Cochran-Armitage Trend Test: To assess linear associations between ordinal measures (e.g., RPS class) and binary outcomes.
Survival Analysis: Kaplan-Meier curves and Cox regression models were used to determine hazard ratios (HR) for ESKD progression based on NDKD status.
Multiple Testing Correction: X² tests utilized the Benjamini-Hochberg correction for categorical variables, while continuous variables were analyzed via t-tests or Kruskal-Wallis tests as appropriate.
Results
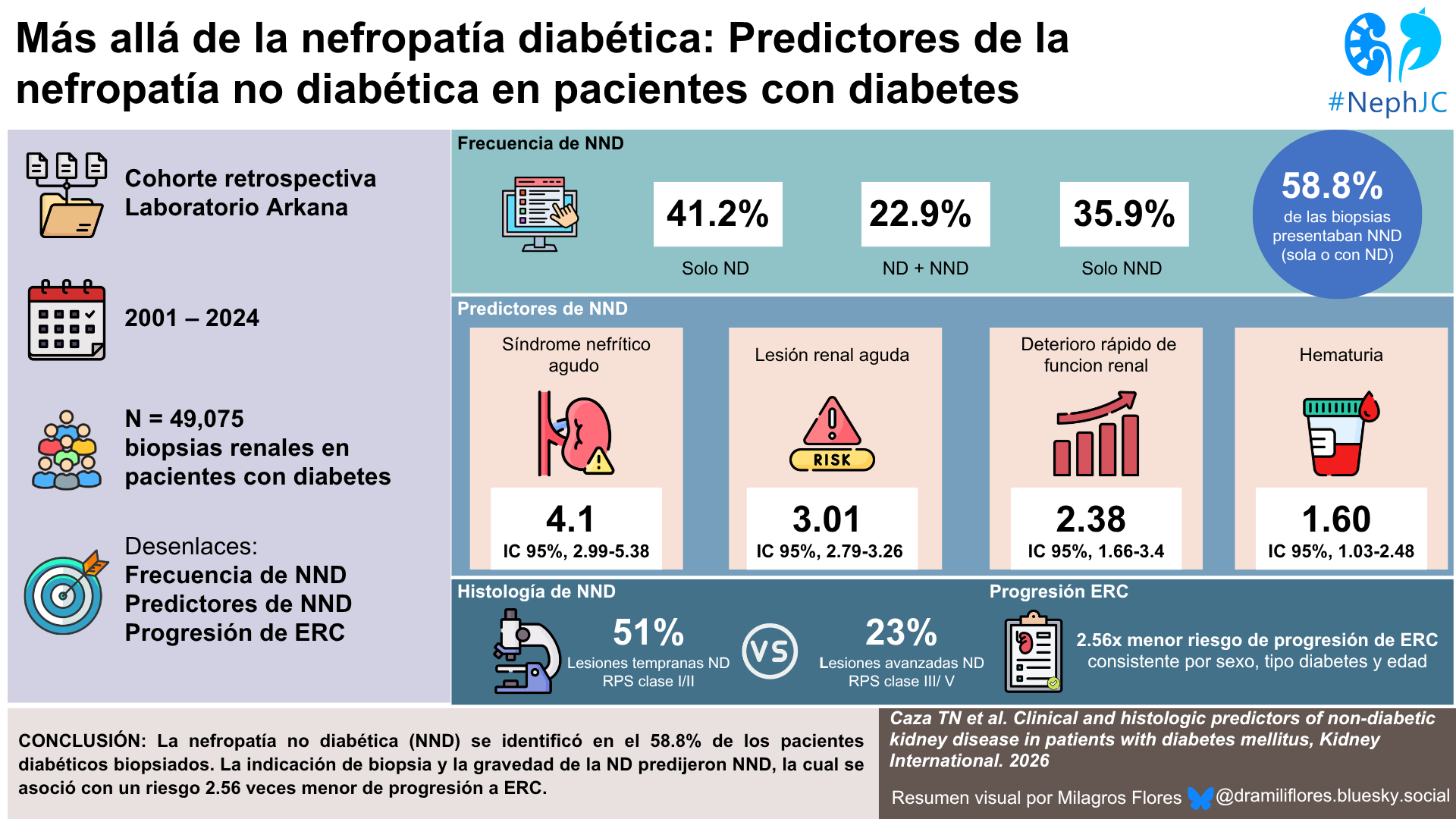
The cohort included 49,075 kidney biopsies from patients with diabetes analyzed between 2001 and 2024. Among biopsied patients, DN alone was present in 41.2%, 22.9% had DN and concurrent NDKD, and 35.9% had isolated NDKD(not 18.3% as erroneously mentioned at one place in the article describing cohort characteristics), resulting in an overall NDKD prevalence of 58.8% of all biopsies. Patients with NDKD were more frequently biopsied in the inpatient setting and more commonly had positive autoimmune serologies or concurrent infections. A second cohort of 13,995 patients with biopsy-proven DN and documented biopsy indications was subsequently analyzed to assess predictive variables of concurrent NDKD. Mean age was 58.5 years, with male predominance in all three diagnostic categories. Among patients with known diabetes type, 83.2% had T2DM. Hypertension and obesity were significantly more common in patients with DN alone.
Overall the most prevalent NDKD diagnoses included acute tubular injury (ATI), acute interstitial nephritis (AIN), proliferative glomerulonephritis, IgA nephropathy (IgAN), and crescentic glomerulonephritis. ATI was the most common diagnosis in both the cohort with DKD + NDKD and those with NDKD, the most frequent concurrent diagnoses were ATI, IgAN, and AIN, while in isolated NDKD, the most common findings included ATI, arterionephrosclerosis, membranoproliferative glomerulonephritis (MPGN), crescentic glomerulonephritis, focal segmental glomerulosclerosis (FSGS), and IgA nephropathy. The biopsy incidence of DN has steadily increased over time, from 7% of native renal biopsies between 2001–2007 to 17% between 2015–2022.
Table 1. NDKD diagnoses in patients with diabetes mellitus with and without concurrent DN. Caza TN et al, Kidney Int, 2026
The highest odds of concurrent NDKD diagnosis was associated with acute nephritic syndrome in a 59% (OR 4.01, 95% CI 2.99 to 5.38), followed by rapidly progressive renal failure (OR 2.38, 95% CI 1.66 to 3.4), acute kidney injury (OR 3.01, 95% CI 2.79 to 3.26), and hematuria (OR 1.60, 95% CI 1.03 to 2.48). Meanwhile, proteinuria (17%) as well as CKD (9%) were associated with the lowest diagnostic yield, making DN alone the most probable diagnosis in these clinical settings.
Common second diagnoses in patients with DN as per clinical indication were as follows:
AKI: ATI (46%), Infection associated GN, Acute interstitial nephritis
RPRF- crescentic GN (49%), ATI
Acute nephritis- infection associated GN(51%), ATI, crescentic GN
Unexpected increase in proteinuria- ATI(19%), MN , IgAN
Hematuria- IgAN (44%), Infection associated GN
CKD- ATI (32%), IgAN, AIN
Suspicion of NDKD- ATI (18%), Infection associated GN
Kidney biopsies were performed to rule out a specific diagnosis for 19.8% of cases, most commonly for monoclonal gammopathy of renal significance confirmed in only 7% of these patients. Among rule-out biopsies, minimal change disease had the highest diagnostic accuracy (45%), followed by ATI (33%) and membranous nephropathy (30%).
Table 2. Clinical indication for renal biopsy and odds on NDKD diagnosis. Caza TN et al, Kidney Int, 2026
Patients younger than 30 years and older than 60 years had the highest prevalence of NDKD, increasing steadily over 80 years, particularly when diagnosing AKI or acute nephritic syndrome. Black and Hispanic patients were less likely to have an NDKD diagnosis (OR 0.75 and 0.76, respectively), but more frequently demonstrated severe DN on biopsy.
Earlier diabetic nephropathy lesions (RPS class I–II) were associated with higher rates of NDKD compared with advanced diabetic lesions (RPS class III–IV), with a prevalence of 51% versus 23%, respectively. This was a nearly 2-fold difference across almost all clinical indications.
Figure 3. Comparison of class of diabetic glomerulosclerosis on kidney biopsy and frequency of a NDKD. Caza TN et al, Kidney Int, 2026
Among the 13,061 patients who progressed to end-stage kidney disease (ESKD), patients with an NDKD had significantly better kidney outcomes compared with those with DN alone. The presence of DN alone was associated with a markedly higher risk of progression to ESKD compared to those without DN (HR 2.56; 95% CI 2.45 to 2.68), and this association held across sex, diabetes type, and age groups.
Figure 4 from Caza et al, KIR 2026. Kaplan-Meier survival analysis demonstrating the impact of a nondiabetic kidney disease (NDKD) on renal survival in patients with diabetes mellitus with and without diabetic nephropathy (DN)
Discussion
This large retrospective cohort of 49,075 kidney biopsies represents the most comprehensive analysis to date examining the prevalence and predictors of NDKD in diabetic patients. The authors report that 58.8% of biopsied patients harbored NDKD either alone or concurrent with diabetic nephropathy (DN), broadly consistent with the prior study, in which 36% of patients had isolated NDKD and an additional 27% had concurrent DN and NDKD (Sharma et al,,CJASN, 2013).
How should we interpret this finding? Do these data suggest that most diabetic patients with kidney disease require biopsy, or do they instead demonstrate that biopsy selection strongly determines diagnostic yield? The striking heterogeneity in NDKD prevalence across studies, ranging from 3% to 82.9% —is likely explained by differences in patient selection and biopsy thresholds (Fiorentino M et al, NDT 2017). For instance, those who prospectively biopsied consecutive patients with moderate CKD and/or significant proteinuria regardless of clinical suspicion, reported only 33.6% NDKD (18.2% NDKD alone +15.4% NDKD+DKD) (Basu et al, BMJ Open Diabetes Res Care, 2022); while those who biopsied based on multiple atypical indications, reported a higher NDKD prevalence of 74.9% (64% NDKD +10.1% DKD+NDKD)(Sakaci T et al, Clin Nephrol, 2024).
One of the most clinically relevant findings of this study is the multiple clinical parameters examined as potential predictors of NDKD. Patients presenting with AKI, rapidly progressive kidney dysfunction, or hematuria had markedly higher odds of harboring NDKD. These findings reinforce the evidence from prior studies and meta-analyses suggesting that acute or inflammatory presentations should prompt consideration of kidney biopsy in diabetic patients, particularly when the clinical trajectory appears inconsistent with classic diabetic nephropathy (Sreedharan S et al, Cureus, 2026 | Sakaci T et al, Clin Nephrol, 2024 | Bermejo et al, Nefrologia, 2024| Vignesh S et al, Indian Journal of Kidney Diseases, 2024 | Chemouny et al, AJN, 2021| Bermejo et al, Nefrologia, 2016).
The histologic findings further emphasize the heterogeneity of kidney disease in diabetes. Notably, ATI and AIN emerged among the highest scores of NDKD, findings that were less prominently reported in earlier biopsy cohorts (Sharma et al, CJASN, 2013). Interestingly, this distribution differs from prior studies in which glomerular diseases such as FSGS predominated among NDKD diagnoses (Sreedharan S et al, Cureu, 2026 | Sakaci T et al, Clin Nephrol, 2024 | Vignesh S et al, Indian Journal of Kidney Diseases, 2024| Bermejo et al, Nefrologia, 2016). This discrepancy may reflect differences in biopsy practices, including the broader inclusion of inpatient biopsies and patients presenting with acute kidney injury or inflammatory syndromes in the current study. Taken together, these findings suggest that contemporary diabetic biopsy populations may increasingly capture acute and potentially treatable tubulointerstitial or infection-related pathologies rather than exclusively chronic glomerular diseases.
It is important to note that despite its size and clinical relevance, there are several limitations.
Since this study is a retrospective pathology-based cohort, it is inherently subject to referral and selection bias, such that only patients appropriate for biopsy were included.
Baseline kidney function, longitudinal clinical follow-up, and standardized biopsy criteria were unavailable for many patients. Moreover, the evolution of diabetes therapies and changes in biopsy practice over the two-decade study period may also have impacted both biopsy indications and histologic findings.
Although the KDIGO 2020 Diabetes in CKD guideline recognizes uncertainty of atypical presentations, it does not provide specific recommendations regarding when kidney biopsy should be pursued in diabetic patients. This study highlights the need for systematic and integrated biopsy frameworks that combine clinical features, rather than isolated predictors alone (Gesualdo et al, CKJ 2023).
This study does offer compelling evidence that kidney disease in diabetics is more heterogeneous than commonly appreciated. These findings challenge the traditional assumption that progressive renal dysfunction in diabetes reflects DN alone, and calls for a more individualized approach to kidney biopsy consideration. In particular, the observation that patients with NDKD demonstrated significantly lower risk of progression to ESKD reinforces the clinical value of obtaining a tissue diagnosis when atypical features are present.
Conclusion
In a time of precision nephrology, this study suggests that kidney biopsy is still considered one of the most useful diagnostic techniques applicable to diagnose the existence and the presence of unexplained or non-classic kidney disease in diabetics.
Summary by
Reviewed by
Header designed by AI and prompts from Brian Rifkin