

#NephJC Chat
Wednesday Sep 27 8 pm BST, 12 noon Pacific
Note day: *Wednesday* Sep 27 9 pm Eastern
2017 Jul 15. pii: S0272-6386(17)30781-3. doi: 10.1053/j.ajkd.2017.05.018. [Epub ahead of print]
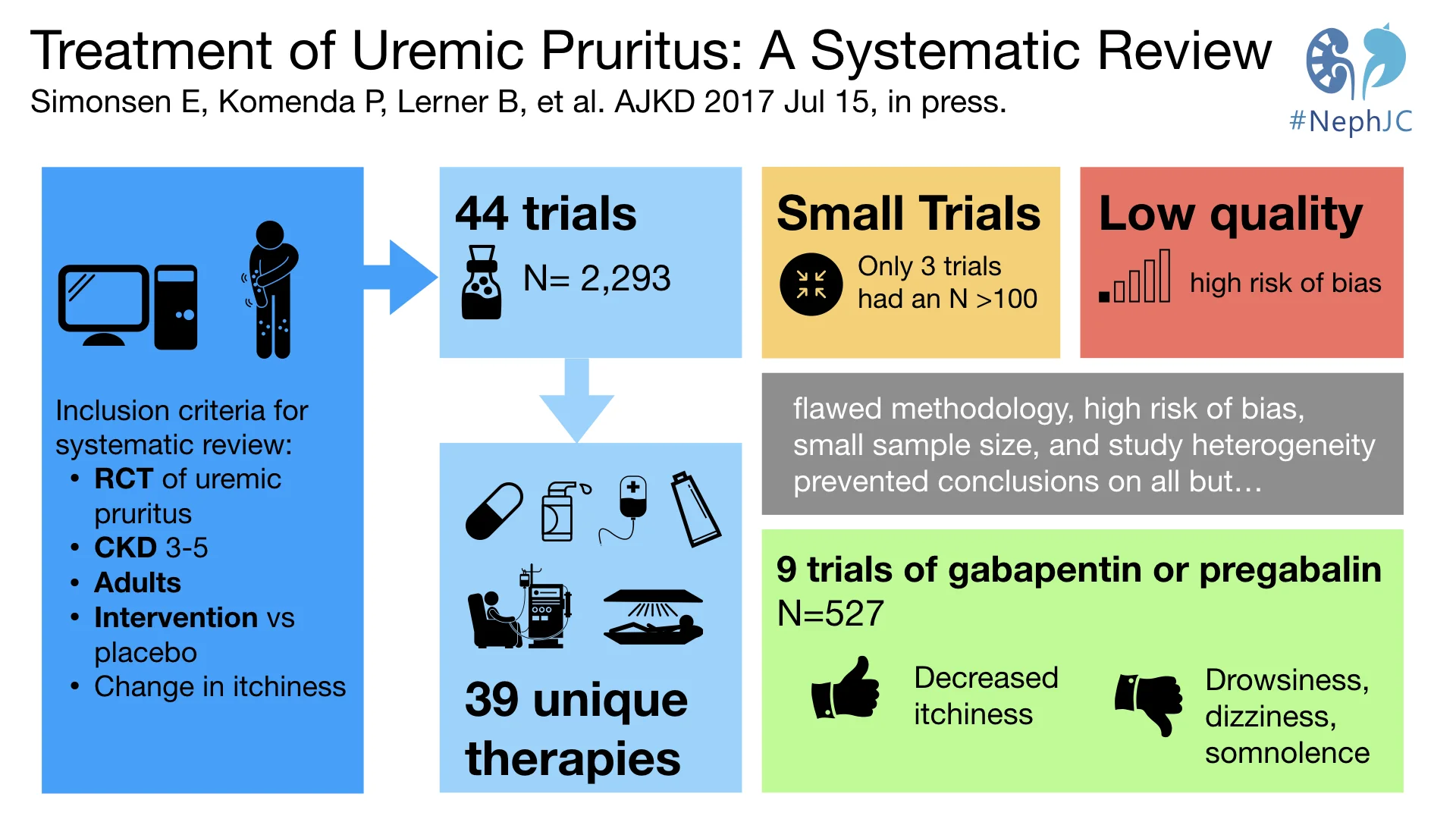
Treatment of Uremic Pruritus: A Systematic Review.
Simonsen E, Komenda P, Lerner B, Askin N, Bohm C, Shaw J, Tangri N, Rigatto C.
PMID: 28720208 Fulltext is Free (at AJKD)


Also read the excellent AJKD blog post from Paul Phelan here
Summary
Background
Itching, harmless - or a minor and irritating symptom as it sounds, can seriously impact quality of life. Especially if it is chronic and doesn't go away - read about some unfortunate cases in this long read from Atul Gawande (go on, click the link, read it and come back. We will wait - and promise it is very good). Patients and caregivers, and to a lesser extent nephrologists, are aware of the pervasive symptom of “itchiness” in those with reduced kidney function. Indeed, it is among the priorities identified by the SONG-HD initiative from the patient perspective. Uremic pruritus affects up to 46% of hemodialysis patients. Eighteen percent find itching to be severe according to a recent DOPPS study. To belabor the point, anywhere from 1 in 5 to as many as 1 in 2 patients have itchiness and we seriously underestimate the problem.
The pruritus is usually symmetric, involving the skin of the back, face and arms. Interestingly it does not exhibit a skin lesion, of course until the scratching begins. Needless to say, the undulating symptom is directly related to a dialysis patient’s quality of life, sleep ability, and is associated with mortality.
The pathophysiology of the pruritus is currently unknown, although there are several hypotheses. Uremic neuropathy and nerve inflammation are possible pathogenic mechanisms. Dry skin, high phosphate levels, and hyperparathyroidism are usual suspects. Increased μ-opioid receptors in chronic kidney disease is also implicated. There are various therapeutic options, with variable efficacy and adverse effects, and teasing these out was the purpose of the current systematic review.
Methods
This was a systematic review limited to randomized controlled trials of patients with CKD stage 3 or higher, comparing any intervention versus placebo, and targeting pruritis. The outcome was an assessment of pruritis, which is usually done with a quantitative change in pruritus intensity on a visual analogue, verbal, or numerical rating scale. Not surprisingly, there was considerable heterogeneity in design, treatments, and outcome measures, which did not allow for a quantitative synthesis in the form of a meta-analysis.
Results
Study Selection
One hundred and fourteen trials were identified as suitable for review out of 823 records. Forty-four met criteria set out for inclusion. The overall patient sample size totaled 2,293 patients with 39 different therapies. Most trials were small in size with only 3 including more than 100 patients. All studies included patients 16 years or older. Additionally, every study included hemodialysis patients with 3 studies containing peritoneal dialysis patients. Because pruritus is a subjective complaint, patients rated their symptoms on a visual, verbal, or numerical scale.

Figure 1 from Simonsen et al, AJKD 2017
Interventions
The most popular and successful treatments historically have been with the medications gabapentin and pregabalin. Nine trials used one or both of these medications. These trials showed a statistical significance for the medication when compared to placebo. None of the trials examined long-term effects, with the longest trial last only 12 weeks. Common side effects of these neuromodulators included drowsiness, dizziness, and somnolence.
Other interventions with more than 1 or 2 trials were mast cell stabilizers, phototherapy, and dialysis prescription changes.
Given the 39 different treatment comparators, there was a wide range of effectiveness. Treatments that include a statistical significance of symptoms compared to placebo or control included: cromolyn sodium, oral zinc, broadband UV-B light, high-flux hemodialysis, high-permeability hemodialysis, montelukast, nalfurafine hydrochloride, cholestyramine, thalidomide, GLA-enriched cream, capsaicin cream, pramoxine lotion, “Chinese herbal” cream, and acupressure. These positive outcomes have not been compared to each other robustly enough to recommend one treatment over the other.
Treatments that did not show a statistical significance included: There was a significant risk of bias - and trial reporting was such that this was unclear in many cases (see figures 2 and 3 from the article for details).
Discussion
The authors and this #NephJC reviewer agree that quantifying effectiveness of each treatment is highly selective and subject to bias. Given the variety of symptoms and treatments leading to improvement, a positive or negative outcome is highly variable. Use of these treatments is almost impossible to do with blinding. Patient blinding between acupuncture and pill based therapy is impossible without direct comparison.
Side effects were also varied and relative to the treatment prescribed. Very few patients or providers would be surprised that sunburn or tanning occurred with UV light therapy.
Currently in the ESRD community it is most accepted that gabapentin is the “leading” effective therapy with the most amount of trial data. The other 38 treatments studied are also effective in many patients, indicating that repeated transitioning of therapies is appropriate when relief is not achieved with monotherapy.
We welcome the experience with each of these treatments and the subjective biases of physicians, providers and patients in this debilitating condition.
Questions to ponder for our #NephJC: How do you feel the authors addressed bias? Do diabetic patients with neuropathy have less pruritus given their large exposure to gabapentin treatment? Do patients in sunny climates like Florida have less pruritus than Canadians given the increased exposure to UV light? What are your patients telling you on dialysis rounds?